External Defibrillator
Background
An external defibrillator is a device that delivers an electric shock to the heart through the chest wall. This shock helps restore the heart to a regular, healthy rhythm. The device is generally sold as a kit that consists of a power control unit, paddle electrodes, and various accessories. The parts are made individually and pieced together via an integrated production process. Since then medical device manufacturers have introduced various defibrillators, internal and external, that have added years to patients' lives.
To understand how a defibrillator can restart a stalled heart, the physiology of the organ must be considered. The human heart has four chambers, which create two pumps. The right pump receives the oxygen-depleted blood returning from the body and pumps it to the lungs. The left pump receives the oxygenated blood from the lungs and pumps it to the rest of the body. Both pumps have a ventricle chamber and an atrium chamber and operate in a similar manner. The blood collects in the atrium and is then transferred to the ventricle. Upon contraction, the ventricle pumps the blood away from the heart.
The coordination of the pumping action is critical for the heart to function correctly. A pacemaker region, which is located in the heart's right atrium, is responsible for this control. In this region, a spontaneous electrical impulse is created by the diffusion of calcium ions, sodium ions, and potassium ions across the cell membranes. The impulse thus created is transferred to the atrium chambers causing them to contract, pushing blood into the ventricles. After about 150 milliseconds the impulse moves to the ventricles, which causes them to contract and pump blood out of the heart. As the impulse moves away from the chambers of the heart, these sections relax. In a normal heart, the process then repeats itself.
In some cases, the electrical control system of the heart malfunctions and results in an irregular heart beat such as ventricular fibrillation. Various conditions can cause ventricular fibrillation including blocked arteries, poor reaction to anesthesia, and electrical shock. Defibrillators are used to supply a strong electrical shock to the heart. Two electrodes are placed on the chest and a shock is given. A typical defibrillator device will deliver a shock for three to nine milliseconds. For reasons not quite understood, the shock essentially resets the natural ventricular rhythm and allows the heart to beat normally.
In practice, an external defibrillator can be operated at an emergency site or a hospital. The operator first turns on the machine and then applies a conductive gel to the paddle electrodes or patient's chest. The energy level is selected and the instrument is charged. The paddles are placed firmly on the patient's unclothed chest with a pressure of about 25 lb (11 kg). The buttons on the electrodes are pressed simultaneously and the electric shock is delivered. The patient is then monitored for a regular heartbeat. The process is repeated if necessary.
History
The discovery that a misfiring heart could be restarted using an electrical charge is one of the great developments of modern medicine. This idea was begun around 1888 when it was suggested by Mac William that ventricular fibrillation might be the cause of sudden death. Ventricular fibrillation is a condition in which the heart suddenly beats irregularly, preventing its blood-pumping ability that ultimately can lead to death. It can be caused by a coronary artery blockage, various anesthesia, and electric shock.
In 1899, Prevost and Batelli made the crucial discovery that large voltages applied across the heart could stop ventricular fibrillation in animals. Various other scientists studied further the effects of electricity on the heart during the early nineteenth century.
During the 1920s and 1930s, research in this field was supported by the power companies because electric shock induced ventricular fibrillation killed many power utility line workers. Hooker, William B. Kouwenhoven, and Orthello Langworthy produced one of the first successes of this research. In 1933, they published the results of an experiment, which demonstrated that an internally applied alternating current could be used to produce a counter shock that reversed ventricle fibrillation in dogs.
In 1947, Dr. Claude Beck reported the first successful human defibrillation. During a surgery, Beck saw his patient experiencing a ventricular fibrillation. He applied a 60 Hz alternating current and was able to stabilize the heartbeat. The patient lived and the defibrillator was born. In 1954, Kouwenhoven and William Milnor demonstrated the first closed chest defibrillation on a dog. This work involved the application of electrodes to the chest wall to deliver the necessary electric counter shock. In 1956, Paul Zoll used the ideas learned from Kouwenhoven and performed the first successful external defibrillation of a human.

William Bennett Kouwenhoven was born January 13, 1886 in Brooklyn. Trained as an electrical engineer, his most enduring contributions to science came from the medical arena. Using his electrical engineering background, Kouwenhoven invented three different defibrillators and developed cardiopulmonary resuscitation (CPR) techniques.
In the 1920s, Kouwenhoven's interest crossed between electrical engineering and medicine. His engineering work focused on high tension wire transmission of electricity. Kouwenhoven became interested in electricity's possible role in reviving animals. He knew that when applied to the heart an electric current could start it again.
From 1928 through the mid-1950s, Kouwenhoven developed three defibrillators: the open-chest defibrillator, the Hopkins AC Defibrillator, and then Mine Safety Portable. These were intended for use within two minutes of the start of ventricular fibrillation, and at least one required direct contact with the heart. In 1956, Kouwenhoven began developing a non-invasive method. During an experiment on a dog, he realized the weight of the defibrillator's paddles raised the animal's blood pressure. Based on this Kouwenhoven developed CPR.
By the early 1960s, CPR was being used throughout the United States. Kouwenhoven's ground-breaking work was recognized by the medical community and the electrical engineering establishment. He was awarded the American Medical Association's (AMAj Ludwig Hekton Gold medal in 1961 and 1972, and the American Institute of Electrical Engineering's Edi-son Medal in 1962. Johns Hopkins bestowed Kouwenhoven with an honorary M.D. in 1969 (he is the only person to ever receive this honor). He won the Albert Lasker Clinical Research Award in 1973. Kouwenhoven died on November 10, 1975.
In the 1960s, scientists discovered that direct current defibrillators had fewer adverse side effects and were more effective than alternating current defibrillators. In 1967, Pantridge and Geddes demonstrated that using a mobile, battery-powered DC defibrillator could save lives. The late sixties saw the introduction of an implantable defibrillator by Dr. Michael Mirowski. Both internal and external defibrillators were redesigned in the 1970s to automatically detect ventricular fibrillation. As improvements in electronics and computers became available these technologies were adapted to defibrillators.
Today, defibrillation has become an integral part of the emergency response routine. In fact, the American Heart Association considers defibrillation a basic life support skill for paramedics and rescue workers.
Raw Materials
Biocompatible raw materials must be used in the construction of defibrillators because they interact with patients. The materials must also be pharmacologically inert, nontoxic, sterilizable, and functional in a variety of environmental conditions. The various parts of the defibrillator, including the control box casing, microelectronics, and the electrodes, are all made with biocompatible materials. Typically, the casing is made of a hard polystyrene plastic or lightweight metal alloy. The electrodes are made from titanium and silicone rubber. The microelectronics are made of modified silicon semiconductors. The primary materials used in battery construction can include numerous compounds such as lead acid, nickel-cadmium, zinc, lithium, sulfur dioxide, and manganese dioxide.
Design
The basic design of a external defibrillator includes a control box, a power source, delivery electrodes, cables, and connectors. While these devices are sometimes implanted in patients, this work focuses on portable units used in hospitals and emergency sites.
Controls
The control box is a small, lightweight, plastic case. It contains the power generating and storage circuits. In general, the charge that is delivered to the patient is generated by high voltage generation circuits from energy stored in a capacitor bank in the control box. The capacitor bank can hold up to 7 kV of electricity. The shock that can be delivered from this system can be anywhere from 30-400 joules. The control box also houses the control electronics and the operator input buttons. The typical controls on a defibrillator control box include a power control button, an energy select control, a charge button, and an energy discharge button. Certain defibrillators have special controls for internal paddles or disposable electrodes.
Electrodes
The electrodes are the components through which the defibrillator delivers energy to the patient's heart. Many types of electrodes are available including hand-held paddles, internal paddles, and self-adhesive, pre-gelled disposable electrodes. In general, disposable electrodes are preferred in emergency settings because they have advantages such as increasing the speed of shock and improving defibrillation technique. The paddle size affects the current flow. Larger paddles create a lower resistance and allow more current to reach the heart. Thus, larger paddles are more desirable. Most manufacturers offer adult paddles, which are between 3.1-5.1 in (8-13 cm) in diameter, and pediatric paddles, which are smaller.
Since skin is a poor conductor of electricity, a gel must be used between the electrode and the patient. Without this conductor, the level of the current reaching the heart would be reduced. Also, the skin may be burned. A variety of gels and pastes are available for this purpose. These are composed of cosmetic ingredients like lanolin or petrolatum. Chloride ions in the formula also help form a conductive bridge between the skin and the electrode allowing better charge transfer. Many of these materials are the same compounds used for other medical devices such as ECG scans.
Battery
Batteries are essentially containers of chemical reactions. In defibrillators, a variety of batteries are used. They are characterized by the chemical reactions contained in them and include lead-acid, lithium, and nickel-cadmium systems. These batteries can typically be recharged by an outside power source, and when not in use defibrillators are stored plugged in. Since extreme temperatures negatively affect the batteries, defibrillators are stored in controlled environments. Over time batteries wear out and are replaced. This is important because battery chemistries are inherently corrosive and potentially toxic.
Automated external defibrillators
In 1978, the automated external defibrillator was introduced. This device is equipped with sensors that are applied to the chest and determine whether ventricular fibrillation is actually occurring. If detected, the device calls out instructions to deliver an electrical shock. These automated devices greatly reduce the training required to use a defibrillator and have saved thousands of lives.
The Manufacturing
Process
Defibrillators are sophisticated electronic devices. Typically, manufacturers rely heavily on suppliers to produce the component parts. These parts are then shipped to the manufacturer and pieced together to form the final product. The process is therefore not linear but an integrated one.
Making the batteries
- 1 One type of battery used in defibrillators is a lithium battery. The design of this type of battery involves the connection of multiple cells. For defibrillators, the cells are made up of lithium metal and sulfur dioxide gas. Working under oxygen free conditions, the lithium is shaped into a solid case and sulfur dioxide is added.
- 2 The cell is then hermetically sealed to prevent the sulfur dioxide gas from escaping and moisture from entering. In one battery design, four of these lithium cells are wired in series and packed in a solid housing. An 8-amp fuse is mounted to each cell for safety reasons. All of the cells have a vent that can be used to release pressure if it builds up too high.
Creating the casing
- 3 To make the casing and the outer housing for the electrodes, a process known as injection molding may be used. In this procedure plastic pellets are melted and forced into shape. The pellets of plastic are put into a holding bin attached to the injection-molding machine and melted.
-
4 The material is then passed through a hydraulically controlled screw.
As the screw rotates, the plastic melts further. It is directed through
a nozzle and injected into the mold. The mold is made up of two metal
halves that form the shape of the part when brought together. When the
plastic is in the mold, it is held under pressure for a moment and then
cooled. As it cools, the plastic hardens and takes on the shape of the
mold.
The mold pieces are separated and the plastic part falls out onto a conveyor. The mold then closes again and the process is repeated. After the plastic parts are ejected from the mold, they are manually inspected.
 An external defibrillator kit.
An external defibrillator kit.
Making the electronics
- 5 The motherboard inside the casing contains all the electrical circuitry of the defibrillator including semiconductor chips, resistors, capacitors, and other devices. Using an intricate method known as hybridization, these components are combined to form a single complex circuit. Construction begins with a small board that has the electronic circuit configuration printout out on it.
- 6 The board is then moved through a computerized machine that places the appropriate components exactly where they are needed on the board. This action is accomplished by a placing head on the device. It holds the electronic component and presses it down on the board.
- 7 The electronic components are then affixed to the board by a soldering machine using a minimum number of welds. The circuitry is allowed to cool and is tested before being connected to the control box casing.
Assembly
-
8 The electronic boards are manually attached to the casing by line
workers under extremely clean conditions. The boards are
attached with various screws and fasteners. The casings are fitted with control buttons and metal electrode adapters. The whole assembly is closed with screws and sent to an area for testing and final packaging.
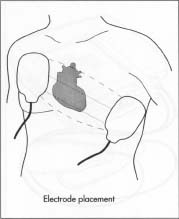 The positioning of the defibrillator's paddles.
The positioning of the defibrillator's paddles.
Making paddle electrodes
- 9 In addition to the outer shell, the paddle electrodes are made up of a metal plate and a cable that connects them to the main machine. The metal plate is a conducting alloy such as tin. The plate is made using a machine called a "continuous caster." The caster converts molten tin to thin sheets by forcing it between large, water cooled rollers. A thin layer of stannous chloride is sprayed on the sheets, and they are cut into the appropriate size for the electrode.
- 10 The cable is produced by a drawing technique. In this step, metal is heated until it softens. It is then rolled out and drawn to produce a long wire.
- 11 The wire is then cut and bundled with other wires. The bundle of wires are coated with a relatively thick polymeric insulator and wrapped in an insulating sheath. One end of the wire is soldered to the metal plate.
- 12 The plate is then manually fitted onto the outer shell and the cable is fed through a hole in the back of the shell.
- 13 The end of the cable is fitted with an adapter that can be plugged into the control box.
Final assembly
- 14 When all of the components are completed, they are brought together in a final packaging. Line workers take the individual parts of the machine including the electrodes, battery, and control box and put them in a cushioned box. They also include cables, instruction manuals, and other information.
- 15 Before any product is shipped, it is tested to ensure that it delivers the proper charge.
Quality Control
Making visual and electrical inspections throughout the entire production process ensures the quality of each defibrillator. Electronic circuit fabrication is particularly sensitive to contamination so production is done in air-flow controlled, clean rooms. The clothes worn by line assembly workers must be lint-free to help reduce the chance of contamination. Since the batteries are critical and potentially dangerous, they are subjected to extensive performance, safety, and stability testing. The functional performance of each completed defibrillator is tested to make sure it works. This can be accomplished by charging the battery, discharging the device, and measuring the charge output. To simulate real-life use, these tests are done under differing environmental conditions. Quality testing is also done routinely after the defibrillators are purchased. Engineering personnel perform maintenance checks every three to six months depending on usage. This typically involves a charge-discharge test.
Each company that manufactures medical devices is required to register with the United States Food and Drug Administration (FDA). They must adhere to the FDA's quality standards known as "good manufacturing practices." This requires extensive record keeping procedures and also subjects the manufacturer to routine inspection of the facility for compliance.
The Future
In the future, defibrillators will be improved to become safer and more efficient. For ex-ample, designers are continually improving the electrode design to reduce the chances that the device operator will get shocked. A recent patent issued in the United States describes an electrode system that uses a Y shaped cable for just this purpose. Advances in the fabrication of integrated circuits will also make the devices easier to use and more lightweight.
Another important area of improvement will be found in battery technology. Scientists at the United States Department of Energy's Brookhaven National Laboratory have patented a new metal alloy that should greatly improve rechargeable battery performance. The alloy can be incorporated into a nickel/metal hydride battery to provide a significant increase in capacity for storing charge. In addition to these areas of advancement, improvements in defibrillator design such as the incorporation of more sensors to give vital information about a patient's condition will also be introduced.
Where to Learn More
Books
Carr, J. J. Introduction to Biomedical Equipment Technology. 2nd ed. Prentice Hall Career and Technology, 1993.
Fox, Stuart. Human Physiology. W. C. B. Publishers, 1990.
Oever, R. V. D. Cardiac Pacing and Electrophysiology: A Bridge to the 21 st Century . Kluwer Acedemic Publishers, 1994.
Periodicals
Shakespeare, C. F., and A. J. Camin. "Electrophysiology, Pacing, and Arrhythmia." Clinical Cardiology 15 (1992): 601-606.
Other
Worthington, Janet Farrar. "The Engineer Who Could." Hopkins Medical News. 18 March 1998. 2 October 2001. < http://www.hopkinsmedicine.org/hmn >.
Perry Romanowski
For school I've got to make an essay about whether public area's should be required by law of having AED's. But I've got a question. What is really happening during the defibrillation? How is the energy transfered through the handles and how does it defibrillate the patient?
I'm sorry for my English, hopefully you'll understand it.
Thank you very much,
Niels Visser